

Background: Follicular lymphoma is the second most frequent non-Hodgkin lymphoma (NHL) accounting for 20-25% of NHL cases in western countries. Although it has an indolent character, progressive disease or relapse occurs within first two years following therapy initiation in ~20% of FL cases. Several somatic mutations were identified in genes of epigenetic regulation or other biological processes by sequencing of FL tumors. Current diagnostic and prognostic evaluations include invasive methodologies that may be less effective and more risky for the FL patients. Therefore, there is urgent need for development of non-invasive methods to improve diagnosis as well as risk stratification. Accumulating evidence has shown that circulating cell-free DNA (cfDNA) includes tumor-derived mutations in several cancer types; however, this possibility has not been comprehensively investigated in FL patients. Here we evaluated the potential diagnostic and prognostic value of cfDNA in FL cases by addressing the proportion by which cfDNA samples contains cancer-associated and prognosis-related mutations.
Methods: Twenty FL cases with available clinic data were included in this study. Thirteen of these cases were symptomatic who were later treated with R-chemo whereas rest of the cases were asymptomatic who were in watchful-waiting. Plasma cfDNA, granulocyte DNA, and FFPE tumor tissue DNA samples were obtained from treatment-naive FL cases. A custom gene panel including exons and exon-intron boundaries of 110 FL-associated genes was constructed based on previously published studies for ultra-deep targeted sequencing. Paired-end sequencing of the captured regions were performed using a HiSeq system in Novogene, which generated 150 bp NGS reads. Targeted genomic regions were covered with > 1500X average effective sequencing depth for identification of somatic variants with low variant allele fractions (VAF). Variants present in cfDNA and tumor tissue DNA but not in patient-matched granulocyte DNA were identified with the GATK pipeline including the MuTect2 variant caller. Somatic variants associated with hematopoietic and lymphoid tissues in the COSMIC database were chosen for further analyses. The final high-confident list of variants was determined by visual investigation and through additional filtering of each variant using Integrative Genomics Viewer. Selected variants were cross-validated with Sanger sequencing. Survival analyses were performed with Survival and Survminer R packages.
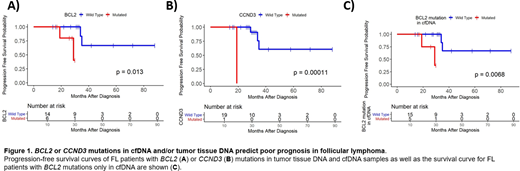
Results: Ultra-deep targeted sequencing revealed 91 somatic variants (71 missense, 12 nonsense, 4 indel, 4 splice site) in 31 genes included in the panel. Consistent with previous reports, the most frequently mutated genes were CREBBP (40%), BCL2 (30%), STAT6 (25%), EZH2 (20%), and CARD11 (20%). In symptomatic cases, 41.5% of the variants was present in both cfDNA and tumor tissue DNA, whereas 52.3% and 6.2% of them was present only in tumor tissue DNA or in cfDNA samples, respectively. In asymptomatic cases, 11.5% of the detected variants was present in both cfDNA and tumor tissue DNA, while 84.6% and 3.8% of them were in only tumor tissue DNA or cfDNA samples. Mutations previously reported to be associated with FL pathogenesis (e.g. KMT2D R2417*) were in the list of common variants observed in both cfDNA and tumor tissue DNA. We observed high Ki67 staining, elevated LDH levels, presence of BCL2 or CCND3 mutations to be significantly associated with progression-free survival (Figure 1A, B). Importantly, survival analysis by stratifying patients based on BCL2 mutations present only in cfDNA also predicted poor prognosis (Figure 1C). One of the FL patient who had progressive disease contained histological transformation-associated gene (i.e. B2M and BTG1) mutations only in the cfDNA but not in tumor tissue DNA sample. Finally, we cross-validated the selected somatic variants with VAF >20% using Sanger sequencing, which showed 100% consistency with NGS results.
Conclusions: Tumor tissue-derived mutations can be detected in most FL patients albeit to a lesser extent than those in DLBCL. Plasma cfDNA genotyping may be useful for improving diagnosis and prognosis especially in symptomatic FL patients. Given that some somatic mutations associated with disease progression are detected only in plasma cfDNA samples, cfDNA genotyping may be useful for choosing appropriate therapy for high-risk FL patients.
No relevant conflicts of interest to declare.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal